Introduction
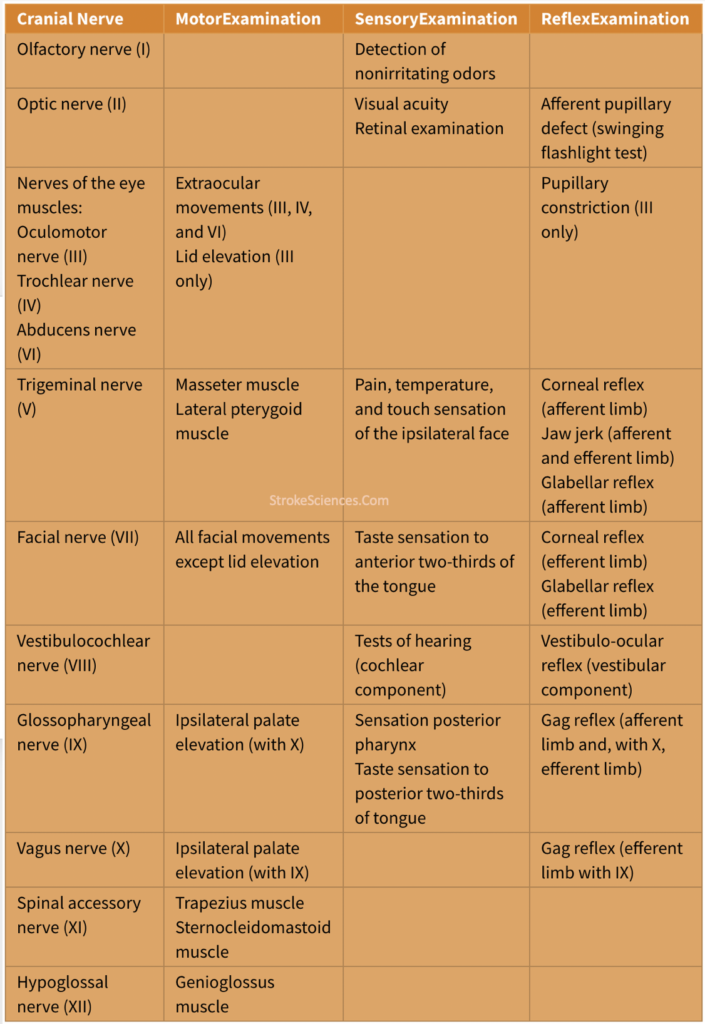
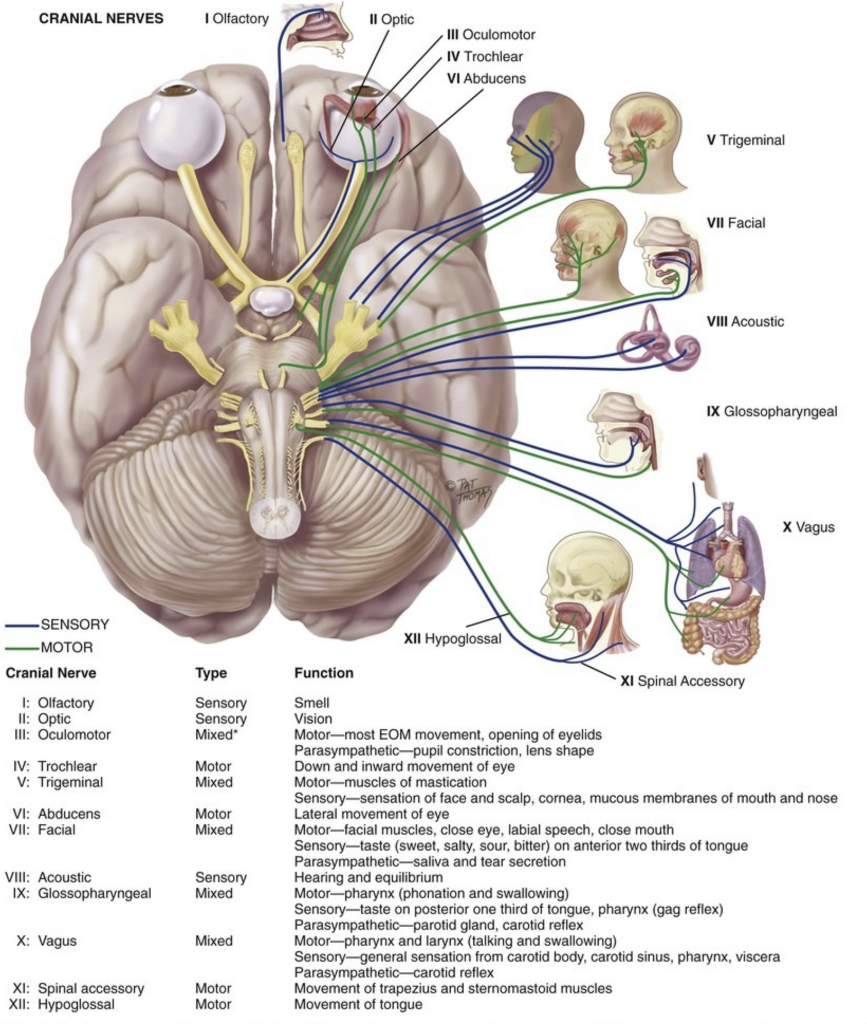
Whether in stroke or other neurological disorders cranial nerves can provide important information about the neurologic functions of the head and neck regions. Cranial nerve (CN) abnormalities not only provide information about a specific nerve but also about the brainstem which houses the nuclei of the CNs and in some cases provide information about the cerebral hemispheres which are the final recipients of incoming sensory information from the CNs such as taste, smell, vision, hearing, and facial sensation. This also proves to be important in CNs involved in descending motor control. Here, all 12 CNs are discussed and approaches to examining them are provided. You can download the table at the bottom.
CN 1: Olfactory Nerve
It is involved in the sense of smell from the nose to the inferior frontal lobe and the medial temporal lobes (olfactory bulb). It is important to note that this is the only sensory modality that sends information directly to the cortex without going through the thalamus. With that being said, testing CN1 tests both the smell and the sensory cortex .
Test: Many neurologists first ask the patient if they have noticed any changes in their sense of smell. Carrying around pocket-sized vials of vanilla and peppermint is also common.
CN 2: Optic Nerve
The optic nerve transmits visual information from the retina to the occipital cortex. It also transmits information about light to the midbrain as the afferent limb of the pupillary light reflex (PLR). PLR tests CN2 (afferent), CN3 (efferent) as well as the midbrain nuclei and the pathways connecting them together.
Test: testing visual acuity (using a snellen chart) and visual fields give information about the eyes, optic nerves, visual cortex and the pathways connecting them together.
CNs 3, 4, 6: Oculomotor Nerve, Trochlear Nerve, Abducens Nerve
The oculomotor nerve (CN3), trochlear nerve (CN4) , and the abducens nerve (CN6) control the movements of the eyes. CN3 also controls elevation of the eyelid and constriction of the pupil.
Test: testing eye movements examine these three nerves and their connections in the brainstem. The ability to follow instructions to look in a specific direction (saccades) and to follow the examiner’s finger (smooth pursuit) requires communications between these brainstem pathways, the cerebellum and the cortical eye fields.
CN 5: Trigeminal Nerve
The trigeminal nerve transmits facial sensation to the sensory cortex via the brainstem and ventral posterior medial nucleus of the thalamus, and also controls the muscles of involved in chewing (mastication).
Test: testing facial sensation including light touch, temperature and pain and evaluation of the strength of jaw opening and closure will provide information about the trigeminal nerve, its nuclei in the brainstem and the sensory and motor regions with which they communicate in the the cerebral hemispheres. More specifically the ventral posteromedial (VPM) nucleus of the thalamus and the postcentral gyrus (sensory strip) for facial sensation; precentral gyrus (motor strip) for motor supply to the muscles of the jaw. The trigeminal nerve also carries the afferent limb of the corneal reflex in response to stimulation of the cornea. This nerve carries both the afferent and efferent limbs of the jaw jerk reflex as well.
CN 7: Facial Nerve
The main function of the facial nerve is to control the movements of facial musculature.
Test: asking the patient to raise the eyebrows and close the eyes tightly tests the upper facial muscles, and asking to smile tests the lower facial muscles. Differences in patterns of facial weakness with respect to the upper and lower face can help localize the site of dysfunction to the facial nerve itself or the motor cortex and the descending pathways controlling such movements.
CN 8: Vestibulocochlear Nerve
The vestibulocochlear nerve is responsible for transmitting auditory and vestibular information to the brain.
Test: The auditory aspect of CN8 is tested by assessing hearing in both ears, which tests the integrity of the pathway from the inner ear, through the nerve and the brainstem, thalamus, and the auditory cortex in the temporal lobes (Heschle’s gyri). The vestibular portion and its brainstem connections with the eye movement nuclei can be assessed by various maneuvers notably the head impulse test where the vestibulo-ocular reflex is tested.
CN 9, 10: Glossopharyngeal Nerve and Vagus Nerve
Both the glossopharyngeal and the vagus nerve have a number of roles including innervation of the muscles of the larynx, pharynx, and afferent and efferent visceral autonomic functions. Dysfunction may cause difficulty with articulation of speech “dysarthria“, decreased speech volume “hypophonia“and difficulty swallowing “dysphagia“.
Test: aside from testing for dysarthria and hypophonia, these two cranial nerves can only be tested by assessing palate elevation (primarily a function of CN 10) and the gag reflex which the afferent limb is supplied primarily by CN9 and efferent limb primarily by CN10.
CN 11: Spinal Accessory Nerve
The spinal accessory nerve controls the trapezius muscle involved in shoulder elevation and the sternocleidomastoid muscle involved in turning head. CN 1 and 11 are the only cranial nerves that do not make contact with the brainstem. CN 11 comprised of spinal roots, but exits the skull with other cranial nerves through the jugular foramen.
Test: To test CN 11 simply ask the patient to shrug their shoulders and turn head side to side.
CN 12: Hypoglossal Nerve
The hypoglossal nerve controls the muscles of the tongue. Like CN 7 and CN 5, its motor control comes from the motor cortex, therefore weakness of the tongue on one side can localize anywhere along the pathway from the contralateral motor cortex to its connections with the CN 12 nucleus in the medulla to the hypoglossal nerve itself.
Test: It is assessed by moving the tongue. Observing tongue deviation can confirm contralateral lesions in the central nervous system or nerve damage.